
All About your Pelvic Floor
"DO YOUR KEGELS!" SEEMS TO BE THE PREGNANT WOMAN'S MANTRA,
BUT ARE KEGELS THE BEST THING FOR THEM?
HOW MUCH DO YOU REALLY KNOW ABOUT YOUR PELVIC FLOOR?
Ah, the pelvic floor. Such an exciting topic, and we can't talk about this fun part of you without addressing STRESS URINARY INCONTINENCE (SUI) - aka peeing-when-peeing-shouldn't-happen (perhaps a better title for this article?). Right? Because we've all been there. That sneeze/laugh/jump/run oh-shit-moment when you suddenly feel very connected to your 90 year old grandmother, swear you will never have another kid, pray to the pelvic floor gods that it was a small enough leak to not show up on your pants like it does when your 3 year old chooses to play trucks instead of sitting on the potty, all while trying to casually glance (ahem) downthere to investigate the situation without everyone in the Costco lineup looking at you and laughing and pointing and wondering why you don't have a bulk supply of Depends in your cart. We've all been there, right?
Nearly EVERY MUMMA will experience SUI to some degree during and/or after pregnancy. Apologies if this is news to you first-trimester-first-time-mumma-to-be. A whopping 90% of women who experience SUI in the late stages of their pregnancy will have some form of SUI postpartum. Welcome to the MOTHERLAND ladies! Welcome.
YOUR PELVIC FLOOR WILL UNDERGO MORE STRESS, STRAIN AND INJURY THAN ANY OTHER STRUCTURE IN YOUR BODY DURING PREGNANCY AND DELIVERY.
As if what's happening to the rest of you isn't traumatic enough.
This is not a topic to shy away from. Odds are, the hot mumma sweatin' through her jumping jacks next to you in your postnatal fitness class is red in the face not just from the exercise. Odds are she just peed-a-little-when-peeing-shouldn't-happen. IT DOES HAPPEN, BUT IT SHOULDN'T. And it can (should! must!) be fixed.
SO, LET'S TALK ABOUT IT.
Before I formally introduce you to this topic though, you should know that if you are having pelvic issues 1) YOU ARE NOT ALONE, as I just said they are far too common, and 2) while pregnancy and peeing-when-peeing-shouldn't-happen, unfortunately, go hand in hand more often than not, ANY issue down there should not be taken lightly. Issues "down there" include SUI, fecal incontinence, general pelvic pain, vaginal pain, or any other pain, discomfort or issue that doesn't feel quite normal with ANY of your pelvic structures, pelvic floor or other. Regardless of the issue or severity of your symptoms, you should seek help and advice from a professional (doctor, midwife, or physical therapist). This article is not meant to substitute such advice, but to be an adjunct to your understanding and goal for a healthy pelvic floor.
Being a physical therapist, I talk to patients all the time about their pelvic floor function. And although I don't specialize in PF rehabilitation, I did centre my thesis on it and it's connection to our breathing mechanism, so you could say that I know a few things. It really is a fascinating area of our anatomy and one that is connected to just about every inch of the rest of our body. But let's start with some basics.
WHERE IS THE PELVIC FLOOR?
An obvious place to start. I will guarantee that you will optimize your pelvic floor function if you have a little understanding of it's anatomy.
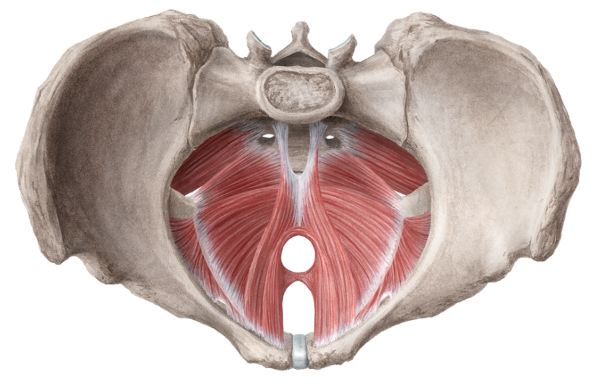
Your pelvic floor is comprised of three layers of muscles (and ligaments, connective tissue (fascia), blood vessels and nerves) that span the floor of your pelvis, which is like a big bowl (see picture above). It attaches to your tail bone and pelvis in the back, and to your pubic bone in the front. Simple as that.
It kinda looks like a hammock between these points.
For the front of the class kids: watch this video on pelvic floor anatomy.

what does it do?
Your pelvic floor has many functions, but the most important is that it acts to keep it all in. It physically supports your bladder and urethra, vagina/cervix/uterus and rectum and their contents (hullo!), against the pressures of gravity, as well as internal pelvic and abdominal pressures (i.e. snnnneeze). Without a properly functioning pelvic floor, those inner structures can head south (aka pelvic organ prolapse), and/or their contents can leak. Not. What. You. Want.

The downward displacement of your pelvic organs is called PELVIC ORGAN PROLAPSE (POP). There are three degrees of POP based on the severity of organ displacement. And since we're laying it all out there, bad news and all, you should know that nearly all vaginal deliveries are associated with a slight downward displacement of the bladder. This is known as a FIRST DEGREE CYSTOCELE. Odds are you won't even know you have this unless your doctor or midwife mention it. And you may or may not have SUI associated with a first degree cystocele postpartum. But it is important to know that things CAN and do move with any pregnancy and delivery (and as we age). It's just how it is. A first degree prolapse may be nothing to worry about and resolve on it's own as tissue tighten back up post delivery, but consider that there are two other degrees that you really don't want to explore.
Is it okay to have pain down there?
No. No it's not. Not during sex. Not during exercise. Not with any daily activities. Not when you pee or poo, or sneeze or cough. No, pain ANYWHERE down there. This is starting to sound like a familiar Dr. Seuss book
ONLY IF you very recently gave birth and are still in the healing stage, may you consider a little pelvic pain normal. If this isn't the case, then talk to your doctor or find a physiotherapist in your area that treats pelvic floor dysfunction. Any body pain should be investigated. There is a reason why we get pain signals. Find out why.
What causes sui?
There are many possible causes of SUI. Mechanical load on the bladder by the expanding uterus and babe above (think watermelon bouncing around on a water balloon), hormonal changes (relaxin in particular), weak muscles, nerve damage or pressure on a nerve from baby, weight gain or a higher BMI (body mass index), vaginal deliveries that cause structural changes to the pelvic floor itself, an increase in the mobility of the pelvic organs (see POP discussed above), body alignment, excessive coughing, digestive and pressures issues.
Lots of players, ladies. Lotsa playas.
Does a C-section exempt me from SUI?
Sorry, C-section mummas, you are not exempt from SUI. Stats indicate little difference in pelvic floor dysfunction between C-section delivery and spontaneous vaginal deliveries. When it comes for pelvic floor health later in life, the stats suggest that pregnancy, not delivery method, is the reason for most dysfunctions. Which reinforces the point that pregnancy (and that comes with it - see above) causes most SUI. There is, however, statistically more pelvic floor dysfunction with vaginal deliveries using instrumentation (i.e. forceps), or if you've had a vaginal delivery in the past - the more babies, the most dysfunction.
Why does SUI happen?
Although this is a generalized and simplistic model for pelvic floor function, this might help you understand when muscles work and when they fail.
There are three resting states that a muscle could be in: too tight, too lax or somewhere in between (ideal resting length). Force production (how well a muscle contracts) is dependent on the length of the resting muscle.
1. TOO TIGHT - When a muscle is shortened (tight), it cannot effectively contract/shorten more to produce force. Not good.
2. TOO LAX - When a muscle is stretched out (lax), it has longer to go to fully contract. Also not good.
3. JUST RIGHT - When in an optimal resting position (somewhere between tight and lax), force production can be maximal. Like a boxer ready to block a punch - arms aren't held out wide (lax) or pulled in too tightly; they are somewhere in between, flexed and ready to go in a flash.
If you want to get super muscle nerdy, check out the graph below. Sarcomeres are the contractile part of muscle fibers. You can see that there is an ideal resting length for sarcomeres for maximal force production. If they are too close together (tight, short muscle) or too stretched out (lax), the force production is lower.

Take home message: you want to your pelvic floor muscles to be in an optimal resting position, not too tight, not too lax, juuuuust right.
Be Goldilocks, ladies.
Not sure where they're at? Talk to a pelvic floor physio.
This is not okay, mummas. I repeat: FOR THE LOVE OF YOUR PELVIC FLOOR, ORGANS AND SANITY this is NOT okay. The gynecologist in the video who says in her "professional opinion it is OKAY to pee during double-unders" should head the f*#@ (pardon me) back to medical school. This is not okay.
If you pee (even a teeny tiny little leak) during ANY exercise, your pelvic floor (specifically your urethral sphincter) is not doing it's job. So don't stress it and the structures it supports further by bouncing around even more.
If it's broke, fix it.
Your 70 year old self will thank you.
Stressing your pelvic floor to the point of failure, is only going to make your problem worse and will potentially create more issues, so goes the typical injury cascade. And worse usually equals longer to fix. Not. What. You. Want.
Fix the issue by working on your pelvic floor and core strength (as directed by your physical therapist) for a few weeks before trying the aggravating (leaking) activity again. Progress back to your high-impact activities slowly and WITHOUT ANY LEAKAGE.
Can you tell I get a wee bit worked up about this one? Just a weeeee bit. This is just SO important.
HOW CAN I FIX SUI?
Ah, the bajillion dollar question.
You obviously can't do much about the hormones or the human growing inside your belly trampolining on your bladder, but you can work on your strength (pelvic floor and core muscles especially) and your body alignment. These two factors MAY TOTALLY ELIMINATE PRE- AND POST-NATNAL SUI. Yay! Totally, completely what you want.
If you go through pregnancy with a weak pelvic floor and core (unfortunately, this is true of the majority of women, so the stats tell us), and neglect your exercises, odds are you are going to hate ragweed season, postnatal exercise class and Amy Poehler.
That said, all of the playas need to be checked off the list: alignment, nerve irritation, scar tissue, breathing irregularities, etc. You need to know if that pelvic floor is lax or tight, or has scar tissue. And that's why, IF YOU ARE HAVING ANY PELVIC ISSUES, you should really, really, really see a physical therapist. Drop me a line if you are in Ottawa and need a referral.
IF SUI CAN BE PREVENTED, WHY IS IT SO COMMON?
Well, until you saw that little plus sign, odds are pelvic floor exercises were something you knew existed, but rarely practiced. Kinda like stretching - we know we should do it, but so few of us do it regularly. And when we do do it, we usually don't do it quite right.
Also, the stats indicate that very few doctors actually check pelvic floor strength during vaginal exams, and if they do they don't do it well - contributing to a lack of awareness and education. And then there are all of the factors that we can't control - hormones, a growing baby + uterus, etc.
And lastly, the "do your Kegels" mantra that most pregnant women hear is just NOT ENOUGH TO GET IT RIGHT. Kegels usually equates to squeezing your pelvic floor muscles as hard as you can, which may in fact be detrimental to their function.
WAIT, SO I SHOULDN'T DO KEGELS?
Dr. Arnold Kegel was the gynaecologist who encouraged repeated pelvic floor muscle contracting and relaxing to manage pelvic floor dysfunctions for men and women. He also invented the perineometer which is a device used to measure the voluntary strength of the pelvic floor muscles.
EVERY MUMMA KNOWS WHAT IT MEANS TO DO A KEGEL:
SQUEEZE AND SQUEEZE SOME MORE!
What's wrong with this? Well, maybe nothing. But for the many, many women with overactive, tight or scarred (no, not scared) pelvic floor muscles it may not be good. These problems may not allow the muscle fibers to contract optimally, generating effective or pain-free force closure. NOT GOOD. Squeezing and squeezing and squeezing (like most do to Kegel) may be detrimental to their function and even make matters worse, or cause more pain.
KEGELS SIMPLIFY THE ATTENTION THAT THIS AREA REQUIRES AND DESERVES.
PLEASE, PLEASE, PLEASE (again), if you are unsure of your pelvic floor abilities, or if things are not improving within 1-2 weeks of trying daily exercises on your own, seek help from a recommended physical therapist. If you are in the Ottawa area send me a message and I'll happily send you a referral.
IN MOST CASES, GUIDED EXERCISES AND ADVICE FROM A PHYSICAL THERAPIST ARETHE BEST SOLUTION TO A HEALTHIER (HAPPIER) PELVIC FLOOR.
In the mean time, stop Kegel'ing, learn how to contract and relax your pelvic floor (follow the link below!), and work on your core strength and posture. You're pelvic floor will thank you.
To sum up:
Know thy self. Understand your pelvic floor and it's function. Have a look if you're so adventurous.
A healthy pelvic floor is one that can CONTRACT and RELAX. Kegels are not enough.
Pregnancy is a major cause of stress urinary incontinence, so says the literature. This doesn't mean that it has to happen. It is preventable, and totally fixable.
Do NOT do exercises that cause incontinence.
Own it mumma.